

Following several high profile reports such as Mid Staffordshire, Southern Health, and most recently the Care Quality Commission’s Learning, candour and accountability, the National Quality Board has developed national guidance on learning from deaths.
There is evidence to suggest that 3% of deaths that occur in healthcare settings could be classed as avoidable (Hogan et al, BMJ Open, 2015). The purpose of the NQB guidance is to support trusts to learn from deaths and identify themes for improvements in care systems through structured case record reviews and, where appropriate, investigations.
The recurrence of problems can be prevented by identifying themes and generating quality improvements for care systems.
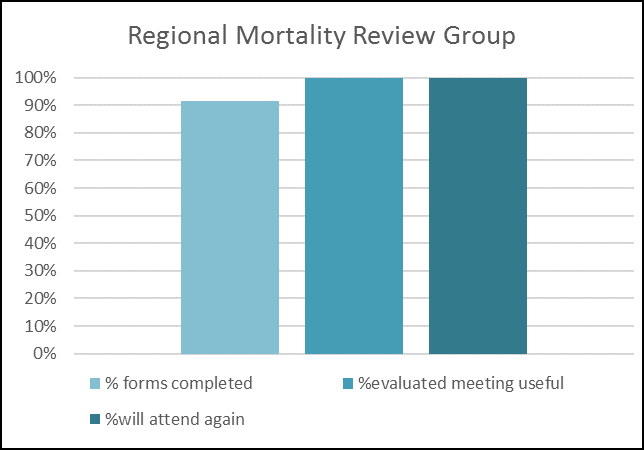
The regional mortality review group brings together clinical and managerial staff from organisations across the healthcare sector, launched in December 2017. This programme aims to improve the standardisation of mortality review processes within community, mental health and secondary care settings and to support the development of quality improvement projects based on the thematic learning from mortality reviews.

Training has already been provided to 52 staff on the Royal College of Physicians’ Structured judgement review tool.
Organisations are also sharing their processes and learning regarding implementation of medical examiners.
The group is also learning from West of England AHSN who were early implementers in structured mortality reviews.
Access more Mortality Review resources here.